When someone sits in front of me and says, “Sometimes I feel like I am having a panic attack, but I am not even scared,” I pay very close attention. This is a sentence I hear often from patients with POTS and other autonomic disorders at California Brain & Spine Center in Calabasas.
Your heart races. You feel lightheaded or disconnected. You might have chest discomfort, shortness of breath, and a sense that something is very wrong. In the emergency room, it is common to be told, “It’s just anxiety” or “You’re having a panic attack.” But for many patients, that is not the full story.
In this article, I want to walk you through the key differences and overlaps between POTS (Postural Orthostatic Tachycardia Syndrome) and panic attacks. My goal is to help you understand why they can feel so similar, how we distinguish them clinically, and why mislabeling POTS as “just anxiety” can delay appropriate care.
“Your symptoms are real. The question is not ‘Is it all in my head?’ The question is, ‘What is the nervous system actually doing, and why?’”
Fast Heart Rate: POTS vs True Panic Attacks
Living with POTS or unexplained episodes of rapid heart rate and dizziness, you might notice:
- Sudden heart racing, especially when you stand up or change position
- Shortness of breath or chest tightness
- Feeling shaky, weak, or “like you might pass out”
- Episodes where your body feels in crisis, even if your mind feels calm
- Being told repeatedly that it is “just panic,” even when it does not feel that way
At California Brain & Spine Center, the team sees many patients who have spent months or years bouncing between cardiology, psychiatry, and urgent care, trying to understand what their episodes really mean. Some have POTS. Some have panic attacks. Some have both, layered on top of each other.
In the sections below, we will outline:
- What POTS is
- What panic attacks are
- How the symptoms overlap
- How they differ in timing, triggers, and physiology
- How the clinic approaches evaluation and treatment when the line between the two feels very blurry
What Is POTS?
POTS, or Postural Orthostatic Tachycardia Syndrome, is a form of dysautonomia. That means the autonomic nervous system – which controls heart rate, blood pressure, and blood vessel tone – is not regulating things smoothly.
In POTS, when you move from lying down to sitting or standing:
- Blood pools in the lower body
- The nervous system struggles to tighten blood vessels fast enough
- The heart compensates by beating much faster (often an increase of 30 beats per minute or more)
- Blood flow to the brain can briefly drop, causing lightheadedness, dizziness, or a near-fainting feeling
Common POTS symptoms include:
- Rapid heart rate with standing
- Dizziness or feeling like you might pass out
- Fatigue and weakness, especially later in the day
- Brain fog, difficulty focusing
- Exercise intolerance
- Sometimes nausea, headaches, or visual changes
The key point: in POTS, position changes and blood flow regulation are central to what your body is experiencing.
What Is a Panic Attack?
A panic attack is a sudden surge of intense fear or discomfort, usually peaking within minutes. It is driven by the brain’s threat detection system, which can misfire even when there is no real danger.
Symptoms can include:
- Rapid heart rate or pounding heartbeat
- Shortness of breath or feeling like you cannot get enough air
- Chest tightness or pain
- Sweating, shaking, or trembling
- Nausea or stomach discomfort
- Feeling unreal or detached (derealization or depersonalization)
- Fear of losing control, going crazy, or dying
Panic attacks often come in waves:
- A trigger or internal sensation is noticed
- The brain interprets it as dangerous
- Adrenaline surges and physical symptoms intensify
- Fear of the symptoms themselves keeps the cycle going
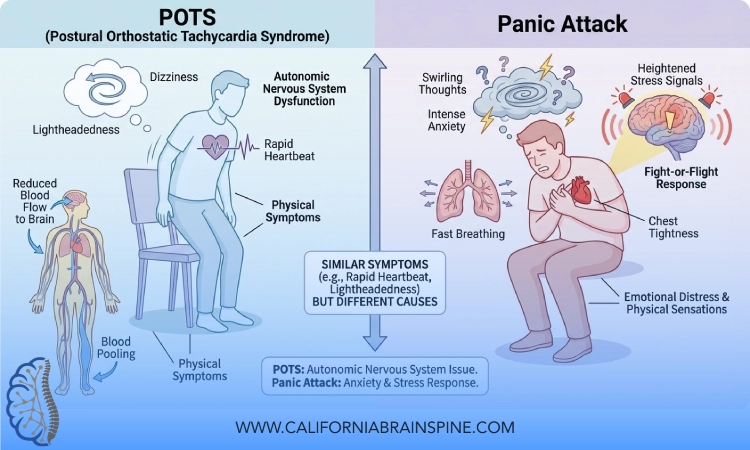
The key point: in panic attacks, the emotional and cognitive experience of fear is central, even if it starts with a physical sensation.
“POTS is driven by a circulation and autonomic regulation problem. Panic is driven by a threat-detection and fear response problem. They both use the same nervous system tools, which is why they can feel so similar.”
Symptoms That Make POTS and Panic Feel the Same
It is not surprising that many patients, and even some clinicians, confuse POTS episodes with panic attacks. The overlap is real:
- Fast heart rate
- Feeling shaky or weak
- Chest discomfort or tightness
- Shortness of breath or “air hunger”
- Dizziness or lightheadedness
- A sense that something is very wrong
The body only has so many ways to signal distress. Whether the trigger is orthostatic stress (standing) or emotional fear, your nervous system will use similar tools: adrenaline, heart rate changes, blood vessel changes, breathing changes.
This is why someone with undiagnosed POTS may end up labeled as “anxious” for years. The symptoms can look like panic, even when the cause is postural and autonomic.
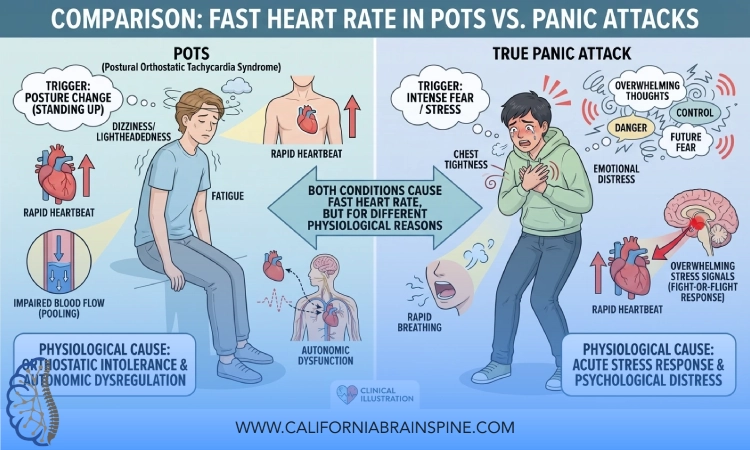
Key Differences: POTS vs Panic Attacks
While the symptoms overlap, there are patterns that help us distinguish POTS episodes from panic attacks.
1. Trigger Patterns
POTS:
- Often triggered or worsened by:
- Standing up
- Prolonged standing
- Hot showers
- Dehydration or missing meals
- Rapid position changes
- Symptoms may improve with:
- Lying down
- Raising the legs
- Slowly changing position
Panic attacks:
- Often triggered by:
- Emotional stress or specific fears
- Sometimes internal sensations that are misinterpreted (a skipped heartbeat, mild dizziness)
- Can occur:
- In any position (sitting, lying, standing)
- Even when externally nothing seems “wrong”
- Not consistently improved just by lying down
If episodes are very strongly tied to standing and orthostatic stress, we are more suspicious of POTS or related autonomic dysfunction.
2. Emotional Experience During the Episode
POTS:
- Patients often say:
- “My heart is racing, but I am not actually panicking.”
- “I feel awful, but my mind is not terrified; my body just feels like it is failing me.”
- Fear can develop over time because of repeated bad experiences, but the initial trigger is usually physical and postural.
Panic attacks:
- Often include:
- Sudden intense fear
- A sense of doom
- Fear of dying, losing control, or going crazy
- The fear is a core part of the episode, not just a reaction afterward.
3. Heart Rate Response to Posture
In clinic, we look carefully at how heart rate changes with position.
POTS pattern (typically):
- Lying: heart rate may be relatively normal
- Standing: heart rate increases significantly (often 30+ bpm within 10 minutes)
- Heart rate elevation is closely linked to upright posture
Panic pattern (typically):
- Heart rate can be elevated in any position
- The rise in heart rate is more tied to surges of anxiety or fear than to standing specifically
This is one reason why structured orthostatic testing is so important when POTS is suspected.
4. Duration and Recovery
POTS:
- Symptoms can build with standing and may persist as long as you remain upright
- Fatigue, brain fog, and lightheadedness can last for hours afterward
- Episodes may be present in milder form much of the day, not only in “attacks”
Panic attacks:
- Often peak within 10 minutes
- Physical intensity usually declines over 20–30 minutes, though exhaustion can linger
- They are often more episodic, coming in discrete bursts
“In POTS, your body is struggling with gravity and blood flow. In panic, your brain is struggling with perceived threat. Both deserve respect and careful evaluation.”
Can You Have Both POTS and Panic Attacks?
Yes. And this is part of what makes the picture so confusing for patients.
Living with POTS can be:
- Unpredictable
- Physically intense
- Isolating
It is entirely understandable that some patients develop secondary anxiety or panic in response to frightening physical episodes, emergency room visits, or ongoing uncertainty about their health.
At California Brain & Spine Center, the team often meets patients who:
- Have clear objective signs of POTS
- Also experience panic attacks, especially in situations that remind them of previous scary episodes
In these cases, treating the autonomic dysregulation and supporting mental health can both be important. The goal is never to dismiss symptoms as “just anxiety” or to overlook genuine panic when it is present.
Why POTS Is So Often Misdiagnosed as Anxiety
Several factors contribute:
- Overlapping symptoms: Fast heart rate, dizziness, and chest discomfort are common in both.
- Normal tests at rest: Traditional heart tests while lying or sitting can appear normal, so clinicians may not see the orthostatic problem.
- Demographics: Many POTS patients are younger women, a group that is unfortunately more likely to have symptoms attributed to stress or anxiety.
- Lack of awareness: Not all clinics are familiar with POTS and other forms of dysautonomia.
The result is that many patients are told:
- “Your heart is fine, so it must be anxiety.”
- “You just need to calm down.”
While mental health support is valuable, this framing can miss the underlying autonomic and circulatory issue, leaving the patient without appropriate evaluation or rehabilitation.
At California Brain & Spine Center, the team’s approach is to validate the symptoms, look for objective patterns, and then build a comprehensive plan rather than stopping at a single label.
How California Brain & Spine Center Evaluates “POTS vs Panic”
When someone comes in unsure whether they have POTS, panic attacks, or both, the evaluation typically includes:
-
Detailed history of episodes:
- What were you doing before symptoms started?
- Were you standing, walking, sitting, or lying down?
- Did you feel fear first, or did physical symptoms come first?
-
Orthostatic vital signs:
- Heart rate and blood pressure lying, sitting, and standing over time
- Relationship between posture and symptom onset
-
Review of other symptoms:
- Brain fog, fatigue, headaches, motion sensitivity, or post-concussion history
- Sleep issues, gastrointestinal symptoms, or temperature regulation problems
-
Screening for mental health symptoms:
- Generalized anxiety
- History of trauma or panic attacks
- How living with symptoms has affected mood and confidence
Based on this, they consider whether:
- POTS or another autonomic disorder is present
- Panic or anxiety is contributing
- Both systems are involved and need to be addressed together
The focus is not on assigning blame but on understanding the full picture of how your nervous system is behaving.
Treatment Principles When POTS and Panic Overlap
Because both POTS and panic involve the autonomic nervous system, treatment often benefits from a dual focus:
1. Supporting Autonomic Stability (For POTS)
In coordination with the patient’s broader medical team, the clinic often helps with:
- Education about POTS and orthostatic triggers
- Hydration and sodium strategies when appropriate
- Compression garments for some patients
- Recumbent-first exercise programs to gently retrain cardiovascular and autonomic responses
- NeuroSensory Integration to address dizziness, visual sensitivity, or post-concussion issues
These steps target the physiological drivers of POTS symptoms.
2. Calming the Threat System (For Panic and Secondary Anxiety)
Even if a patient’s primary issue is POTS, the brain can learn to fear:
- A racing heart
- Dizziness or a “wave” of weakness
- Environments where previous episodes occurred
Supporting the brain’s threat system may include:
- Teaching nervous system-calming breathing and grounding strategies
- Coordinating with mental health professionals for therapy if appropriate
- Reframing episodes so the patient understands what is happening physiologically, which can reduce fear during symptoms
“When patients understand the difference between POTS and panic, they often feel less scared of their own bodies. That alone can soften the intensity of episodes.”
How to Advocate for Yourself if You Are Unsure Which One You Have?
If you are experiencing episodes that feel like panic but you suspect something else is going on, consider:
-
Tracking your symptoms and noting:
- What position you were in
- Whether standing or heat made things worse
- How your heart rate changed (if you have a monitor)
- Whether fear came first or followed the physical sensations
-
Bringing this record to your clinician and asking specifically about:
- POTS or other forms of dysautonomia
- Whether orthostatic vitals can be checked
-
Being honest about mental health:
- If you also feel anxious or have panic, it is helpful information, not something to hide
At California Brain & Spine Center, the team’s goal is to listen and investigate, not to dismiss. The more clearly you can describe your patterns, the easier it is to build an accurate understanding.
FAQ
- How can I tell if my fast heart rate is from POTS or a panic attack?
Look at the context. If your heart races mainly when you stand up or stay upright, and improves when you lie down, POTS is more likely. If the heart racing appears in any position and is closely tied to a sudden wave of fear, panic may be more likely. Many people need formal evaluation to sort this out. - Can POTS cause anxiety?
POTS itself does not “cause” anxiety in the psychological sense, but living with unpredictable and intense physical symptoms can understandably lead to anxiety or even panic. The nervous system is one integrated system; when one part is stressed, others can be affected. - If I have POTS, does that mean my symptoms are not panic attacks?
Not necessarily. Some people have both POTS and true panic attacks. The key is to identify patterns and treat both the autonomic and emotional components where needed, rather than assuming everything is only one or the other. - Why do doctors keep telling me it is just anxiety?
POTS is still under-recognized, and many standard tests done while sitting or lying down are normal. Because the symptoms resemble panic, and because anxiety is common, some clinicians default to that explanation. This is why asking specifically about orthostatic testing and dysautonomia can be important. - How does California Brain & Spine Center approach POTS vs panic?
At California Brain & Spine Center in Calabasas, the team evaluates posture-related patterns, autonomic function, and the broader neuro-sensory picture, while also respecting the role of mental health. They aim to distinguish POTS from panic, identify when both are present, and create a plan that supports the whole nervous system, not just one label.
Conclusion
If your body feels like it is in crisis but your mind is not always afraid, or if you have been told repeatedly that your symptoms are “just panic” while something about that explanation feels incomplete, you are not alone. POTS and panic attacks share many physical sensations, but their underlying causes and patterns can be very different.
From my perspective at California Brain & Spine Center, the most important step is not choosing one label over the other; it is understanding what your nervous system is doing and why. When we identify POTS or other forms of dysautonomia, we can target the autonomic system with recumbent-first exercise, NeuroSensory Integration, and practical daily strategies. When panic or secondary anxiety is also present, we can work alongside mental health support to help your brain feel safer inside your own body.
You deserve more than a quick “it’s just anxiety.” You deserve a careful, respectful evaluation that recognizes the overlap between POTS and panic but also honors their differences. With the right information and a coordinated plan, it is possible to reduce confusion, lower fear, and help your nervous system move toward greater stability.
