When patients come to California Brain & Spine Center in Calabasas with POTS or other forms of dysautonomia, they are often caught in a frustrating cycle. They are told “you need to exercise,” but every time they try, their heart races, they get dizzy or lightheaded, and they feel worse for hours or even days afterward.
As a clinician who works extensively with autonomic nervous system disorders, I see this pattern all the time. The problem is not that your body cannot improve. The problem is that standard exercise advice does not match how a POTS nervous system behaves.
In this article, I will explain why starting with recumbent exercise – rather than jumping straight into upright walking or jogging – is often the most effective, safest, and most sustainable way to rebuild tolerance in POTS. My goal is to help you understand what is happening in your body, reduce fear around movement, and show you how a structured, science-based plan can support your recovery.
“With POTS, the goal is not to push harder. The goal is to train smarter – teaching your autonomic nervous system to trust gravity again, step by step.”
POTS Exercise Guide: Start Recumbent, Not Upright
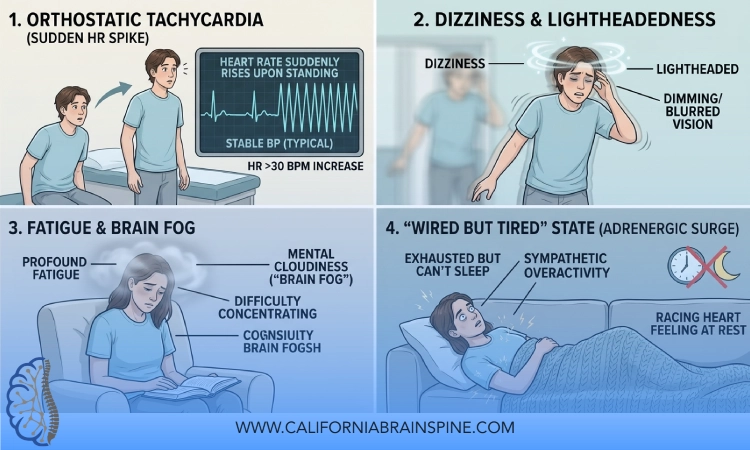
Living with POTS (Postural Orthostatic Tachycardia Syndrome) or related autonomic disorders can make something as simple as standing up feel like a workout:
At California Brain & Spine Center, we see patients who have been told to “just drink more water” or “just walk more,” only to feel worse when they try. The missing piece is often recumbent-first training – using positions that reduce the strain of gravity while still challenging your cardiovascular and autonomic systems in a controlled way.
In the sections below, we will dive into why recumbent exercise works so well for POTS, how we integrate it into a broader brain and autonomic rehab program, and how you can begin to think about movement in a safer, more strategic way.
What Is POTS and Why Does Standing Feel So Hard?
POTS stands for Postural Orthostatic Tachycardia Syndrome. It is a form of dysautonomia, a disorder of the autonomic nervous system – the part of your nervous system that automatically regulates heart rate, blood pressure, blood vessel tone, and blood flow when you change position.
In POTS, when you go from lying down to standing:
- Blood pools in the lower body
- The nervous system struggles to constrict blood vessels quickly and effectively
- The heart compensates by beating much faster (often an increase of 30 beats per minute or more)
- Blood flow to the brain can be temporarily reduced, causing dizziness, lightheadedness, or near-fainting
This is why you might feel:
- More symptomatic when standing or walking
- A little better when lying flat or with your legs elevated
- “Crashed” after even mild upright activity
So, when a POTS patient is told “Just go for a brisk walk every day,” the advice, though well-intentioned, ignores the basic physiology of what is happening when they stand.
This is where recumbent exercise becomes so important.
“In POTS, the problem is not that you are lazy or out of shape. The problem is that your autonomic nervous system is struggling with the simple act of being upright. We must respect that biology.”
Why Traditional Upright Exercise Backfires in POTS?
For someone without POTS, upright exercise like walking, jogging, or using an elliptical is relatively efficient. Their blood vessels constrict appropriately, their heart rate rises in a controlled and proportional way, and their brain continues to receive adequate blood flow.
In POTS, the situation is different:
- Gravity becomes a major stressor. Simply standing is already a challenge for your autonomic nervous system.
- Upright exercise adds another layer of demand. Now your muscles and heart are asking for more blood flow, while your body is already struggling just to keep you from feeling faint.
- The heart rate can spike quickly and excessively. You may see your heart rate jump well above 120–140 beats per minute with minimal effort.
- Symptoms flare: dizziness, nausea, chest discomfort, shortness of breath, brain fog, and extreme fatigue during or after exercise.
This is why many POTS patients report:
- Feeling worse when they try to “exercise like everyone else”
- Developing fear of movement because every attempt ends badly
- Getting labeled as “deconditioned” or “non-compliant” when they simply cannot tolerate standard exercise prescriptions
What is needed is a way to train the cardiovascular and autonomic systems without overwhelming the already fragile upright tolerance. This is the key logic behind recumbent-first programs.
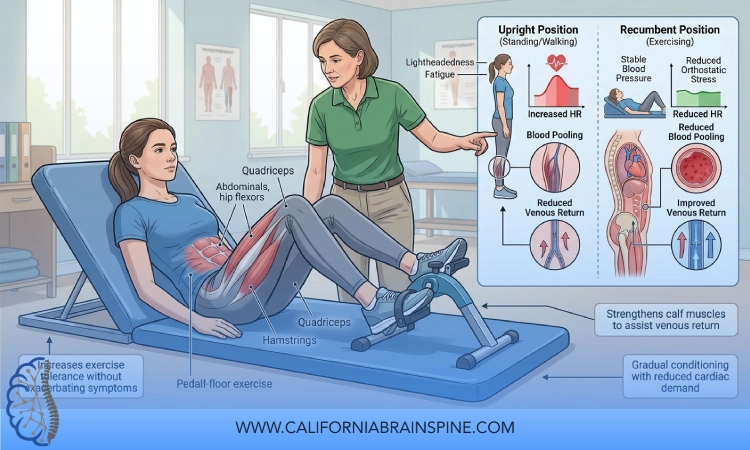
Why Recumbent Exercise First Works for POTS?
Recumbent exercise means exercising in a position where you are partially or fully supported, so your body is not fighting gravity as intensely as it does when standing. Examples include:
- Recumbent bike
- Rowing machine (with careful technique)
- Supine or semi-reclined leg exercises
- Swimming or water-based exercise (depending on individual tolerance)
The core reasons recumbent-first works in POTS:
-
Reduced gravitational load
In a recumbent or semi-reclined position, blood pooling in the legs is reduced. The heart does not need to fight gravity as hard to pump blood back up to the brain. This significantly lowers the risk of dizziness and near-syncope during training.
-
More controlled heart rate response
Because your autonomic system is not battling the full effects of upright posture, your heart rate usually rises more gradually and predictably. This allows you to train within a safe heart rate zone without sudden spikes.
-
Improved tolerance equals consistency
When exercise does not trigger severe symptoms, you are far more likely to stick with it. Consistency is critical for reconditioning your cardiovascular system and supporting autonomic recovery.
-
Neuroplastic training of the autonomic nervous system
By giving the autonomic nervous system repeated exposures to manageable challenge, you encourage neuroplastic changes – gradual improvements in how the system responds to exertion and position changes.
-
Foundation building before upright progression
Once your body and nervous system have adapted to recumbent workloads, we can begin carefully increasing upright time and upright activity without as many crashes.
At California Brain & Spine Center, we use recumbent-first frameworks as part of a larger autonomic rehabilitation and Neuroplasticity Rehabilitation strategy, not as a stand-alone “exercise tip.”
“Recumbent exercise is not ‘cheating.’ It is the logical first step for a nervous system that needs to re-learn how to live safely in gravity.”
How We Structure Recumbent-First Programs for POTS
Every person with POTS is different. Some are significantly deconditioned. Others are high-achieving students or professionals who suddenly find themselves unable to tolerate what used to be normal activity.
In our Calabasas clinic, we personalize exercise progression, but the general principles often look like this:
Phase 1: Stabilization and Baseline Assessment
Before prescribing any exercise, we evaluate:
- Heart rate and blood pressure in different positions (lying, sitting, standing)
- Symptom patterns with posture changes
- Current activity tolerance and crash patterns
- Coexisting issues like concussion, vestibular problems, or brain fog
We also address foundations:
- Hydration and sodium strategies (when appropriate)
- Compression garments if tolerated
- Basic breathing techniques to support autonomic regulation
Only then do we introduce structured recumbent exercise.
Phase 2: Recumbent Cardiovascular Training
We typically start with:
- Recumbent bike or similar device
- Short sessions (for example, 5–10 minutes) at very gentle intensity
- Clear heart rate parameters that reflect the individual’s baseline and triggers
The goals in this phase are:
- Teach the body to tolerate sustained, low-to-moderate effort without major symptom spikes
- Build confidence that movement does not always equal a crash
- Encourage gradual increases in total weekly volume
Over time, as tolerated, we increase:
- Session length (for example, up to 20–30 minutes)
- Slightly the intensity, always in a controlled, stepwise manner
- Frequency (for example, several days per week)
We also monitor how the nervous system responds over the next 24–48 hours, not just during the session. This is crucial in POTS and dysautonomia.
Integrating Strength, Breathing, and NeuroSensory Work
At California Brain & Spine Center, recumbent training is rarely the only focus. We often integrate:
Gentle Strength Training in Supported Positions
- Supine or semi-reclined leg and core work
- Light resistance exercises that do not demand full upright posture
- Gradual focus on muscle endurance in the legs and core, which can help support venous return when standing
Breathing and Autonomic Regulation
POTS and dysautonomia often come with a nervous system that is on high alert. We use specific breathing methods and autonomic regulation tools to:
- Reduce sympathetic overdrive (fight-or-flight)
- Support better heart rate variability
- Teach the body that it can be active without being in crisis mode
NeuroSensory Integration (NSI)
Many POTS patients also have:
- Dizziness with visual stimuli
- Sensitivity to motion, screens, or busy environments
- Overlap with vestibular dysfunction or post-concussion changes
We use NeuroSensory Integration exercises to retrain how the brain integrates visual, vestibular, and body signals. This supports better overall stability and reduces symptom flare-ups during and after activity.
“For POTS patients, exercise alone is not enough. We must train the muscles, the cardiovascular system, and the sensory and autonomic networks together – in a coordinated, patient-centered way.”
When and How We Transition to Upright Exercise
Recumbent-first does not mean recumbent forever. The ultimate goal is to improve your tolerance to upright activities that matter in your daily life:
- Standing and walking
- Attending school or work
- Shopping, social activities, and travel
We typically consider progressing to more upright exercise when:
- You can tolerate recumbent sessions at a reasonable duration without significant symptom crashes
- Your resting and orthostatic heart rate patterns become somewhat more stable
- You feel more confident in your body’s responses
The progression might include:
- Upright cycling on a stationary bike (with careful monitoring)
- Short, structured walking intervals
- Light functional movements like sit-to-stand, step-ups, or gentle incline work
We increase upright activity gradually, always respecting the nervous system’s feedback. If symptoms flare significantly, we may temporarily step back to more recumbent work and refine the plan.
This graded approach is part of how we use Neuroplasticity Rehabilitation to re-train the autonomic nervous system to handle gravity and exertion more efficiently.
A Realistic Case Story: From Bed to Bike to Walking Outside
A young adult patient (details modified for privacy) came to California Brain & Spine Center after a viral illness and subsequent POTS diagnosis. She could stand for only a few minutes before feeling faint. Attempts at “just walking more” left her wiped out for days.
Her evaluation showed:
- Significant heart rate rise on standing
- Marked fatigue and brain fog with minimal upright activity
- Overlap with light dizziness in visually busy spaces
We started with:
- Hydration and sodium strategies guided by her medical team
- Compression stockings when upright
- A few minutes of recumbent cycling at very low intensity, several days per week
At first, even 5 minutes felt like a lot. But because her position was recumbent, she did not crash as severely afterward. Over several weeks, we gradually:
- Increased her recumbent sessions
- Introduced breathing work and NeuroSensory Integration exercises
- Added low-load strength training in supported positions
Months later, she was able to:
- Tolerate 20–30 minutes of recumbent exercise
- Begin short, structured upright walks
- Attend classes part-time again, with better symptom control
This was not a miracle cure or a straight line. It was a structured, patient-centered journey, built around recumbent-first progression and careful autonomic support.
FAQ
- Why is recumbent exercise recommended so often for POTS?
Recumbent exercise reduces the gravitational stress that makes standing so difficult for POTS patients. It allows you to train your cardiovascular and autonomic systems without overwhelming them, making it more likely that you can exercise consistently and safely. - Does recumbent exercise actually improve POTS, or just avoid symptoms?
When used strategically and consistently, recumbent exercise can support long-term reconditioning of the cardiovascular system and neuroplastic adaptation of the autonomic nervous system. It is not just about avoiding symptoms; it is about training your body in a more intelligent way. - How long should I stay with recumbent exercise before moving to upright?
There is no single timeline. Some patients need weeks, others months. The decision depends on how your symptoms, heart rate, and overall function respond. We typically move forward only when you can tolerate recumbent sessions reliably without major post-exertional crashes. - Can I do strength training if I have POTS?
Yes, but it often needs to start in supported positions (lying, semi-reclined, or seated) using light resistance. Strengthening the legs and core can help support venous return and postural stability. The key is gradual progression and close monitoring of your symptoms. - How does California Brain & Spine Center approach POTS differently?
We do not treat POTS as just a heart rate issue. We look at the whole autonomic and neuro-sensory system – including dizziness, brain fog, visual sensitivity, and any history of concussion or vestibular problems. Our plans typically integrate recumbent-first exercise, autonomic regulation, NeuroSensory Integration, and neuroplasticity-based rehabilitation tailored to each patient.
Conclusion
If you live with POTS or another autonomic nervous system disorder, you have probably heard that exercise is important. What you may not have been told is how to exercise in a way that respects your physiology and protects your nervous system from overload.
From my perspective at California Brain & Spine Center in Calabasas, “recumbent first” is not a compromise. It is a strategic starting point – a way to work with your body rather than against it. By reducing gravitational stress, controlling heart rate responses, and integrating autonomic and NeuroSensory Integration work, we can help you build a foundation for more upright activity over time.
You do not have to choose between doing nothing and crashing every time you move. With the right plan, movement can become a tool for healing rather than a trigger for fear.
If you recognize yourself in this story – if you have tried to exercise and only felt worse, or if you are afraid to move because of your POTS symptoms – you deserve a more nuanced, science-based approach. My team and I are here to help you build that plan, step by step, in a way that honors your experience and supports your long-term quality of life.
