How Doctors Diagnose POTS: From Symptoms to Tests
When someone sits across from me and says, “Every time I stand up, my heart takes off and I feel like I might pass out,” I know we have to take their symptoms seriously and systematically. At California Brain & Spine Center in Calabasas, I see many patients who have been told their symptoms are “just anxiety” or “just dehydration,” when in fact they are living with POTS (Postural Orthostatic Tachycardia Syndrome) or another form of dysautonomia.
If you suspect POTS, you may feel:
- Confused by conflicting opinions
- Frustrated by normal test results
- Worried that what you are feeling will not show up “on paper”
My goal in this guide is to walk you through, step by step, how POTS is evaluated and diagnosed, what we look for, and what you can reasonably expect in a careful workup.
“A good POTS evaluation is not just one test. It is a logical sequence: ruling out dangerous conditions, documenting the heart rate response to standing, and understanding the bigger autonomic picture.”
What Exactly Is POTS?
POTS is a form of dysautonomia, meaning the autonomic nervous system does not regulate heart rate, blood vessel tone, and blood flow smoothly, especially when you are upright.
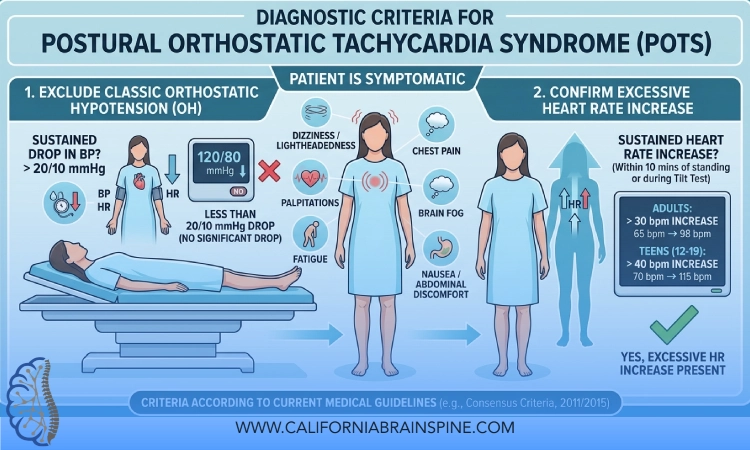
In adults, POTS is generally defined by:
- A sustained increase in heart rate of 30 beats per minute or more (40+ in adolescents)
- Within 10 minutes of standing or head‑up tilt
- Without a significant drop in blood pressure that would indicate classic orthostatic hypotension
- Plus chronic orthostatic symptoms (like dizziness, lightheadedness, palpitations, fatigue) lasting at least 3 months
The diagnosis is both objective (heart rate and blood pressure changes) and clinical (your story and daily symptoms).
Step 1: Listening to Your Story
A careful diagnosis starts with your history, not a machine.
During the initial evaluation, we pay close attention to:
-
Onset:
- Did symptoms start after a viral illness, vaccination, concussion, surgery, or pregnancy?
- Did they appear gradually or suddenly?
-
Typical triggers and patterns:
- Standing up, prolonged standing, hot showers, crowded spaces
- Morning vs evening, during illness, around your menstrual cycle
-
Primary symptoms:
- Dizziness, lightheadedness, near-fainting
- Rapid heart rate, palpitations, chest discomfort
- Brain fog, fatigue, exercise intolerance
- Headaches, GI issues, visual blurring, temperature intolerance
-
Position dependency:
- How you feel lying down, sitting, standing, and walking
- Whether symptoms ease when you lie flat or elevate your legs
-
Previous labels and tests:
- “Anxiety,” “panic,” “deconditioning,” “chronic fatigue”
- Results of prior cardiac, neurological, or endocrine tests
This detailed story helps us decide whether POTS is likely, and what else we must rule out.
Step 2: Basic Physical Exam and Safety Checks
Before focusing narrowly on POTS, we must ensure you are not dealing with something more immediately dangerous.
A basic exam typically includes:
- Heart and lung examination
- Checking for signs of anemia, dehydration, nutritional deficiency
- Neurological screening (eye movements, strength, coordination, sensation, reflexes)
- Observing your balance and gait
- Looking for signs of connective tissue disorders (like joint hypermobility in some patients)
At this stage, the goal is to identify any urgent red flags or clues that point to other conditions that can mimic or coexist with POTS.
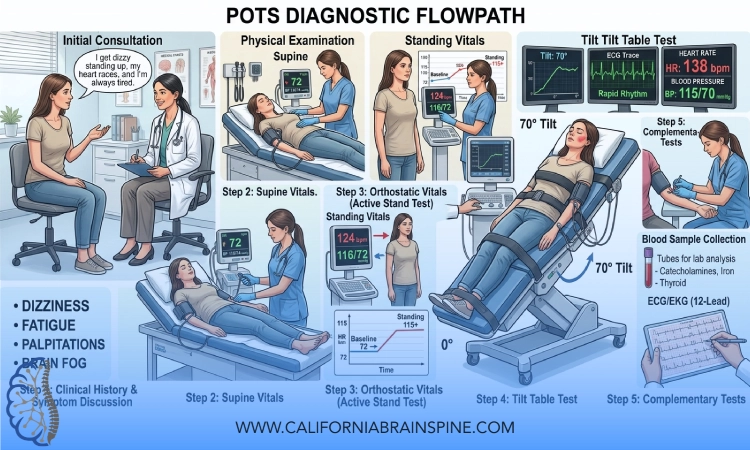
Step 3: Orthostatic Vital Signs – The Core of POTS Testing
The most fundamental diagnostic step is to measure what happens to your heart rate and blood pressure with posture changes.
There are two main approaches:
- A structured active stand test
- A formal tilt table test
In many settings, we start with an active stand test.
Active Stand Test: What We Look For
A typical structured procedure:
-
Resting (supine) phase:
- You lie down quietly for about 5–10 minutes.
- We measure your heart rate and blood pressure at rest.
-
Standing phase:
- You stand up (or are gently brought to standing) and stay still, with support available.
- We measure heart rate and blood pressure at 1, 3, 5, and up to 10 minutes.
- We also note your symptoms in real time: dizziness, palpitations, vision changes, feeling faint.
-
Monitoring for POTS criteria:
- Does your heart rate rise by 30 bpm or more (40+ in adolescents) within 10 minutes of standing?
- Is this increase sustained, not just a brief spike?
- Does blood pressure remain relatively stable (no large drop that would indicate orthostatic hypotension)?
If your heart rate rises significantly with standing and your symptoms match, POTS becomes a strong consideration.
“An accurate POTS diagnosis depends on measuring the right things in the right positions. A normal sitting heart rate does not rule out POTS.”
Step 4: Tilt Table Testing – When and Why It Is Used
A tilt table test is a more controlled version of standing.
You are strapped safely onto a motorized table that tilts you from lying to an upright angle (usually 60–70 degrees), while your heart rate and blood pressure are monitored continuously.
A tilt table test can:
- Document the heart rate rise that meets POTS criteria
- Evaluate for neurocardiogenic syncope, classic orthostatic hypotension, or other autonomic patterns
- Allow controlled observation in a supervised environment if you are prone to near‑fainting
Not every patient needs a tilt table test. In many cases, a well-done active stand test plus history is sufficient. In others, especially more complex or unclear cases, tilt testing helps refine the diagnosis.
Step 5: Ruling Out Other Causes of Tachycardia and Dizziness
POTS is a diagnosis of pattern, not of exclusion only, but we still must make sure nothing else is causing the symptoms.
Common conditions to consider and rule out include:
- Anemia
- Thyroid disorders (hyperthyroidism)
- Cardiac rhythm problems (arrhythmias)
- Structural heart disease
- Severe dehydration or blood loss
- Medication side effects (stimulants, some antidepressants, etc.)
This may involve:
- Blood tests (CBC, metabolic panel, thyroid function, iron studies, sometimes B12, folate)
- ECG (electrocardiogram)
- Possibly echocardiogram or Holter monitoring, depending on your history
The purpose is not to complicate your life but to ensure that your symptoms are not due to a dangerous or treatable cardiac or endocrine pathology that requires a different approach.
Step 6: Identifying Subtypes and Contributing Factors
Once POTS is suspected or confirmed, the next question is: why is your autonomic system struggling?
At California Brain & Spine Center, the team looks for patterns such as:
-
Neuropathic POTS:
- Evidence of impaired nerve control to blood vessels in the legs, leading to excessive pooling.
-
Hyperadrenergic POTS:
- Higher blood pressure or very high heart rate upon standing
- Sometimes associated with elevated norepinephrine levels when upright
-
Hypovolemic POTS:
- Reduced blood volume, often associated with low blood pressure, salt imbalance, or chronic dehydration
-
Post‑viral or post‑infectious POTS:
- Onset after viral illness, sometimes overlapping with long COVID patterns
-
Post‑concussion or neurotrauma-related dysautonomia:
- History of concussion or head/neck injury
- Coexisting dizziness, visual-vestibular mismatch, headaches, or neck involvement
Understanding the subtype or drivers does not change the core diagnostic criteria, but it guides more personalized treatment and rehab planning.
Step 7: Looking Beyond the Heart Rate – The Whole Nervous System
POTS rarely exists in isolation. Many patients also experience:
- Vestibular symptoms (motion sensitivity, vertigo, imbalance)
- Cognitive issues (brain fog, slow processing, memory lapses)
- Headaches or migraines (including vestibular migraine)
- Sleep disturbances
- GI dysmotility, nausea, or abdominal discomfort
- Temperature intolerance and sweating changes
At California Brain & Spine Center, beyond basic POTS criteria, the team often evaluates:
-
Neuro‑vestibular function:
- Eye movements
- Balance systems
- Visual‑vestibular integration
-
Cognitive function:
- Attention, processing speed, working memory
- Impact of upright posture on cognition
-
Autonomic balance:
- Patterns of sympathetic overdrive vs parasympathetic underfunction
- Interaction with breathing patterns and stress responses
This broader view helps distinguish pure POTS from more complex dysautonomia with vestibular, cognitive, or post‑concussion components, and sets the stage for integrative rehabilitation.
Step 8: Documenting Symptom Impact on Daily Life
Diagnosis is not only about numbers; it is also about how much your life is being affected.
Key questions include:
- Can you stand in line at a store without feeling faint?
- How far can you walk before symptoms escalate?
- Can you shower comfortably, or do hot showers trigger episodes?
- How does a typical school or workday feel?
- What activities have you stopped doing because of symptoms?
This helps:
- Confirm that the test results match your reality
- Prioritize what needs the most urgent support
- Build a realistic, stepwise rehabilitation plan
“A heart rate chart alone is not your whole story. We use the data to support you, not to argue with your experience.”
Step 9: Communicating the Diagnosis Clearly
For many patients, finally hearing a clear explanation is a turning point.
A good discussion typically includes:
-
Plain language explanation:
- What POTS is and what it is not
- Why your body reacts this way to standing
- Why symptoms are real, not imagined
-
Differentiating from other labels you may have been given:
- How POTS differs from panic attacks, simple deconditioning, or “just stress”
- When anxiety is secondary, rather than primary
-
Expectations and hope:
- Many patients improve with targeted management and rehabilitation
- Progress is often gradual but meaningful
At California Brain & Spine Center, the team emphasizes that a POTS diagnosis is not the end of the road, but the beginning of a more focused strategy.
Step 10: From Diagnosis to Plan – What Comes Next
Once POTS is diagnosed or strongly suspected, the next phase is building a personalized management plan, which may include:
-
Education and self‑management tools:
- Fluid and salt strategies (when appropriate)
- Compression garments
- Positioning techniques and modified pacing of daily tasks
-
Exercise and rehabilitation framework:
- Recumbent‑first exercise to retrain the autonomic and cardiovascular system without overwhelming you
- Gradual progression to upright activities as tolerated
-
NeuroSensory and vestibular rehabilitation (when relevant):
- Addressing dizziness, motion sensitivity, and visual-vestibular mismatch
- Integrating neuroplasticity‑based protocols
-
Breathing and autonomic regulation techniques:
- Breathing exercises to help stabilize heart rate and blood pressure responses
- Calming sympathetic overdrive
The diagnostic process guides which of these elements are most crucial for you and in what sequence.
Common Questions About POTS Diagnosis
- How long does it usually take to get a diagnosis?
For many patients, years. They are often seen by multiple providers before POTS is considered. With focused evaluation, however, the core diagnostic steps can be completed over a relatively short period, followed by deeper assessment as needed. - Can I have normal tests and still have POTS?
You can have normal cardiac structure, normal resting labs, and a normal ECG, yet still have POTS. The key abnormality often appears only when you are upright. If orthostatic vitals were never checked properly, POTS can be missed. - Do I need a tilt table test to be officially diagnosed?
Not always. A carefully done active stand test with proper heart rate and blood pressure monitoring, combined with your history, is often sufficient. Tilt table testing is reserved for more complex or unclear cases, or when other autonomic disorders are suspected. - Is POTS a psychological condition?
No. POTS is an autonomic nervous system disorder. Anxiety can coexist with POTS, and chronic symptoms can understandably create emotional distress, but POTS itself is not a psychological diagnosis. The evaluation aims to respect both physical and emotional aspects without reducing everything to “just anxiety.”
Conclusion
Being evaluated for POTS is about more than watching your heart rate jump on a monitor. It is about:
- Listening carefully to your story
- Measuring how your body responds to gravity
- Ruling out dangerous or treatable alternatives
- Understanding the broader pattern of autonomic, vestibular, and cognitive symptoms
From my perspective at California Brain & Spine Center, a good POTS diagnosis is both scientific and human. We use structured tests and clear criteria, but we also pay attention to how your life feels day to day. When those align, we can confidently name what is happening and then move into treatment and rehabilitation with a shared, realistic plan.
If your symptoms are dismissed or your testing has never included structured orthostatic measurements, that does not mean “nothing is wrong.” It may simply mean your autonomic system has not been properly evaluated yet. With the right step‑by‑step approach, POTS can be recognized, understood, and actively managed rather than remaining a frightening mystery.
